
Joint Replacement
Phone: 706-839-4096
Shoulder Replacement
Shoulder Replacement video demonstrating Live Intra-operative Computer Assisted Navigation
Reverse Total Shoulder Replacement
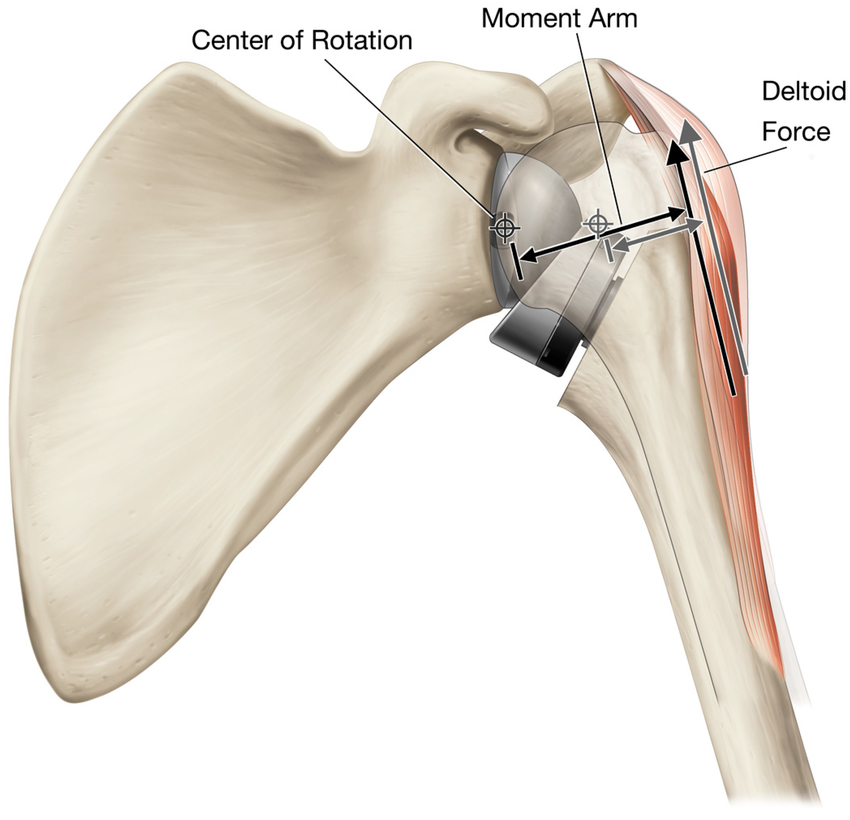
A reverse total shoulder replacement (reverse TSA) is a specific type of shoulder replacement surgery in which the normal ball-and-socket anatomy of the shoulder is reversed: a metal “ball” implant is fixed to the shoulder blade (scapula) and a socket is fixed to the upper arm bone (humerus). This design shifts the shoulder’s center of rotation and allows the deltoid muscle to raise the arm even when the rotator cuff is not functioning.
Why a reverse shoulder replacement is performed
Rotator cuff tear arthropathy: The most common indication. Long-standing, large or irreparable rotator cuff tears lead to shoulder arthritis and loss of active elevation. When the rotator cuff cannot be repaired and the joint is arthritic, reverse TSA restores elevation by relying on the deltoid.
Irreparable massive rotator cuff tears without arthritis: In some patients who have severe pain and loss of function from an irreparable tear but relatively preserved joint surfaces, reverse arthroplasty can improve pain and function.
Complex proximal humerus fractures: In older patients with fractures that cannot be reconstructed reliably, reverse TSA provides predictable pain relief and function.
Failed prior shoulder arthroplasty or revision situations: When a conventional (anatomic) shoulder replacement has failed, or when the rotator cuff is deficient after prior surgery, conversion to a reverse prosthesis is often the solution.
Tumor, infection sequelae, or other complex shoulder conditions where anatomy and soft tissues are not favorable for an anatomic prosthesis.
Who is a good candidate
Patients with severe shoulder pain and loss of function despite appropriate nonoperative care (physical therapy, injections, activity modification, medications).
Patients with rotator cuff tear arthropathy: documented large/irreparable rotator cuff tear plus glenohumeral arthritis and inability to lift the arm.
What to expect before surgery
Evaluation: History, physical exam, and imaging (x-rays; often CT scans to assess bone loss and glenoid wear; MRI if rotator cuff status is unclear).
Preoperative planning: Implant selection and surgical plan based on anatomy and bone quality. You’ll receive anesthesia options and perioperative instructions.
Prehabilitation: Exercises to maximize range of motion and deltoid strength are helpful, and home arrangements should be made for the postoperative period.
What to expect during surgery
Anesthesia: Regional block (interscalene nerve block) and general anesthesia are commonly used for comfort and early pain control.
Procedure length: Typically 1 hour, depending on complexity.
Immediate postoperative care: Pain control with regional block and multimodal analgesia, arm immobilized in a sling, early pain and swelling management.
Recovery and rehabilitation
Same day discharge
Sling: Typically worn for 4 weeks
Physical therapy: Begins early with passive and assisted range-of-motion exercises to prevent stiffness, typically at 2 weeks. Active use and strengthening are started later (often around 4 weeks) as the soft tissues heal.
Timeline:
0–4 weeks: Pain improves steadily; focus on passive motion. Avoid active shoulder elevation against resistance and heavy lifting.
4-8 weeks: Gradual introduction of active range-of-motion and gentle strengthening.
3–6 months: Continued improvement in strength and function; many patients achieve useful functional
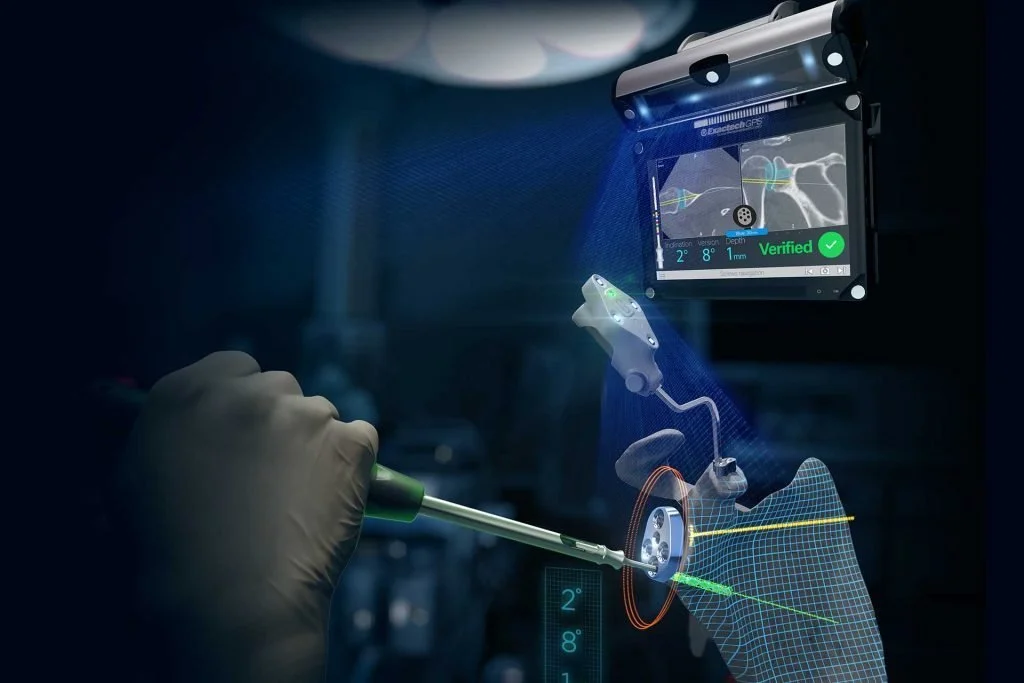
Because the scapula (socket) is a small narrow bone, Dr. Wheeler uses a navigation system from Advita Ortho to help surgeons prepare the bone and place the hardware in precise, preplanned positions during a shoulder replacement.
A CT scan of the shoulder will be performed prior to surgery so that a 3D model of your shoulder can be made. This will allow for precise pre surgical planning to determine the best size & type of implants for your shoulder.
Anatomic Shoulder Replacement
What type of implant is best for you?
For some patients (with large rotator cuff tears, rotator cuff arthropathy, or complex proximal humerus fractures) the reverse total shoulder replacement is the only option. The anatomic shoulder replacement would not work is those situations.
For patients with glenohumeral (shoulder) arthritis, either implant would work. However, the anatomic shoulder replacement requires a functioning/intact rotator cuff to avoid the potential for the implant to dislocate. Patients 55 years old and older, may be better off with a reverse shoulder replacement now, because if their rotator cuff tears later with an anatomic shoulder replacement, another surgery may be necessary to repair the rotator cuff or convert the anatomic implant to a reverse shoulder replacement. If a patient has a reverse shoulder replacement and later in life sustains a tear of the rotator cuff, this should not cause any issues with the implant.
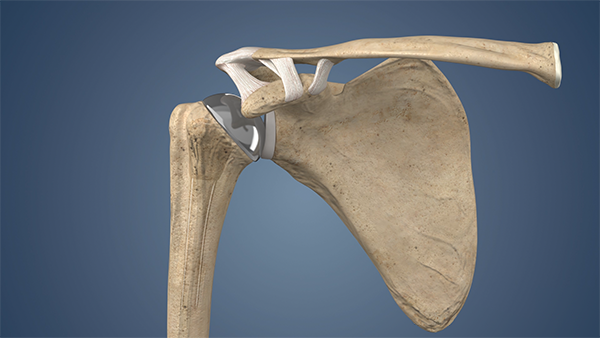
An anatomic shoulder replacement is an operation that replaces the worn parts of your shoulder joint with artificial components that mimic the normal anatomy of the shoulder. The goal is to relieve pain, restore motion, and improve function.
What is replaced
The shoulder joint is made of the ball (head of the upper arm bone, humerus) and the socket (glenoid, part of the shoulder blade).
In an anatomic shoulder replacement the ball is replaced with a smooth metal or ceramic sphere attached to a stem inside the humerus.
The socket is replaced with a plastic (polyethylene) liner fixed to the shoulder blade.
These parts are positioned to reproduce the original ball-and-socket relationship.
What makes it “anatomic”
“Anatomic” means the implant is put in the same positions and orientation as your natural shoulder — the ball on the humerus and the socket on the scapula.
The implant aims to recreate the normal joint shape, alignment, and spacing so the remaining muscles and tendons can work in their usual way.
Why this surgery is done
Severe arthritis (wear-and-tear or inflammatory) that causes persistent shoulder pain and stiffness despite nonoperative treatments (medication, injections, therapy).
Large, but repairable, rotator cuff tendons with joint arthritis in some situations (surgeon will assess cuff quality)..
The intent is to reduce pain, improve range of motion, and restore strength for daily activities.
Who is a good candidate
Patients with intact or mostly functional rotator cuff tendons and severe joint surface damage.
What to expect
Preoperative planning to choose implant size and position.
Surgery typically under general anesthesia; hospital stay may be same day
Rehabilitation follows a staged plan: initial protection, controlled motion, then strengthening.
Most patients see significant pain relief and better use of the arm, though full recovery can take several months.
What to expect during surgery
Anesthesia: Regional block (interscalene nerve block) and general anesthesia are commonly used for comfort and early pain control.
Procedure length: Typically 1 hour, depending on complexity.
Immediate postoperative care: Pain control with regional block and multimodal analgesia, arm immobilized in a sling, early pain and swelling management.
Recovery and rehabilitation
Same day discharge
Sling: Typically worn for 4 weeks
Physical therapy: Begins early with passive and assisted range-of-motion exercises to prevent stiffness, typically within days to 2 weeks. Active use and strengthening are started later (often around 4 weeks) as the soft tissues heal.
Timeline:
0–4 weeks: Pain improves steadily; focus on passive motion. Avoid active shoulder elevation against resistance and heavy lifting.
4-8 weeks: Gradual introduction of active range-of-motion and gentle strengthening.
3–6 months: Continued improvement in strength and function; many patients achieve useful functional
Phone: 706-839-4096

Medial Oblique Incision
2 months post op
Subvastus Total Knee Replacement
A knee replacement is a surgical procedure that restores the function of a damaged knee joint. More precisely, it is better described as knee resurfacing: the surgeon removes small amounts (millimeters) of worn bone and cartilage from the ends of the femur (thigh bone) and tibia (shin bone), and often the back of the patella (kneecap), then places metal and plastic components to recreate smooth, pain-free joint surfaces and proper alignment. The goal is to restore a smooth articulation so you can walk, climb stairs, and return to daily activities with less pain and improved function.
When it’s recommended: Knee replacement is considered only after nonsurgical treatments have failed to control pain and maintain function. Nonsurgical options typically include:
Activity modification and weight loss
Physical therapy and strengthening exercises
Anti-inflammatory medications (NSAIDs) and pain relievers
Corticosteroid injections into the knee
Viscosupplementation (hyaluronic acid) injections
Bracing and orthotics
Assistive devices (canes, walkers)
Who is a candidate: Patients with persistent, severe pain or disability from arthritis (usually osteoarthritis, sometimes inflammatory or post-traumatic arthritis) despite the above measures are candidates for knee replacement/resurfacing. Other considerations include deformity, instability, and impact on quality of life.
The operation and what to expect
Anesthesia: regional (spinal) or general anesthesia, often with nerve block for postoperative pain control.
Resurfacing: the surgeon removes a few millimeters of bone and cartilage and fits metal components to the femur and tibia, plus a plastic spacer to recreate the joint surface. The patella may be resurfaced selectively.
Duration: typically 35-45 minutes.
Recovery:
Most patients go home the same day (outpatient procedure). Overnight stay may be recommended for patients with significant medical problems, inadequate home support, or living alone without help.
Pain control uses multimodal methods: nerve block, oral medications, and ice.
Early motion: physical therapy begins the day of or after surgery. Walking with a walker or cane and range-of-motion exercises start immediately.
Typical timeline:
First 1–2 weeks: manage pain, control swelling, continue walking with assistive device as advised, begin home or outpatient physical therapy.
2 weeks: most patients walk with minimal or no assistive device and perform daily activities with less pain.
1-2 months: substantial improvement in pain and function; many return to low-impact activities.
3-4 months: full recovery of strength and endurance; final results of surgery are apparent.
Risks and longevity: All surgery carries risks: infection, blood clots, stiffness, nerve or vessel injury, ongoing pain, and need for revision surgery. Modern implants and techniques typically last 20–25 years or longer depending on activity level, body weight, and implant type.
Bottom line: Knee replacement is effectively a resurfacing procedure that removes small amounts of damaged bone and cartilage to create smooth joint surfaces. It is reserved for patients whose pain and disability persist despite nonsurgical treatments. Recovery is progressive, and most patients are safely treated as outpatients unless medical or social reasons require observation. Your surgeon will review individualized risks, expected outcomes, and the rehabilitation plan before proceeding.
Total knee replacement animation
A Different Approach to a Knee Replacement
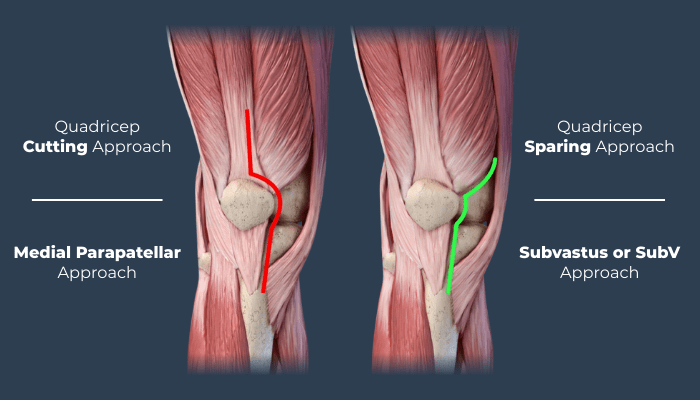
The Subvastus Approach
The Subvastus (also called the medial subvastus) exposure for total knee arthroplasty is a less invasive surgical approach that preserves the quadriceps tendon and fibers of the vastus medialis, in contrast to traditional medial parapatellar or mid-vastus approaches. This preservation leads to less disruption of the extensor mechanism, which can translate into earlier active knee motion, reduced pain with straightening and bending, and often a faster initial functional recovery.


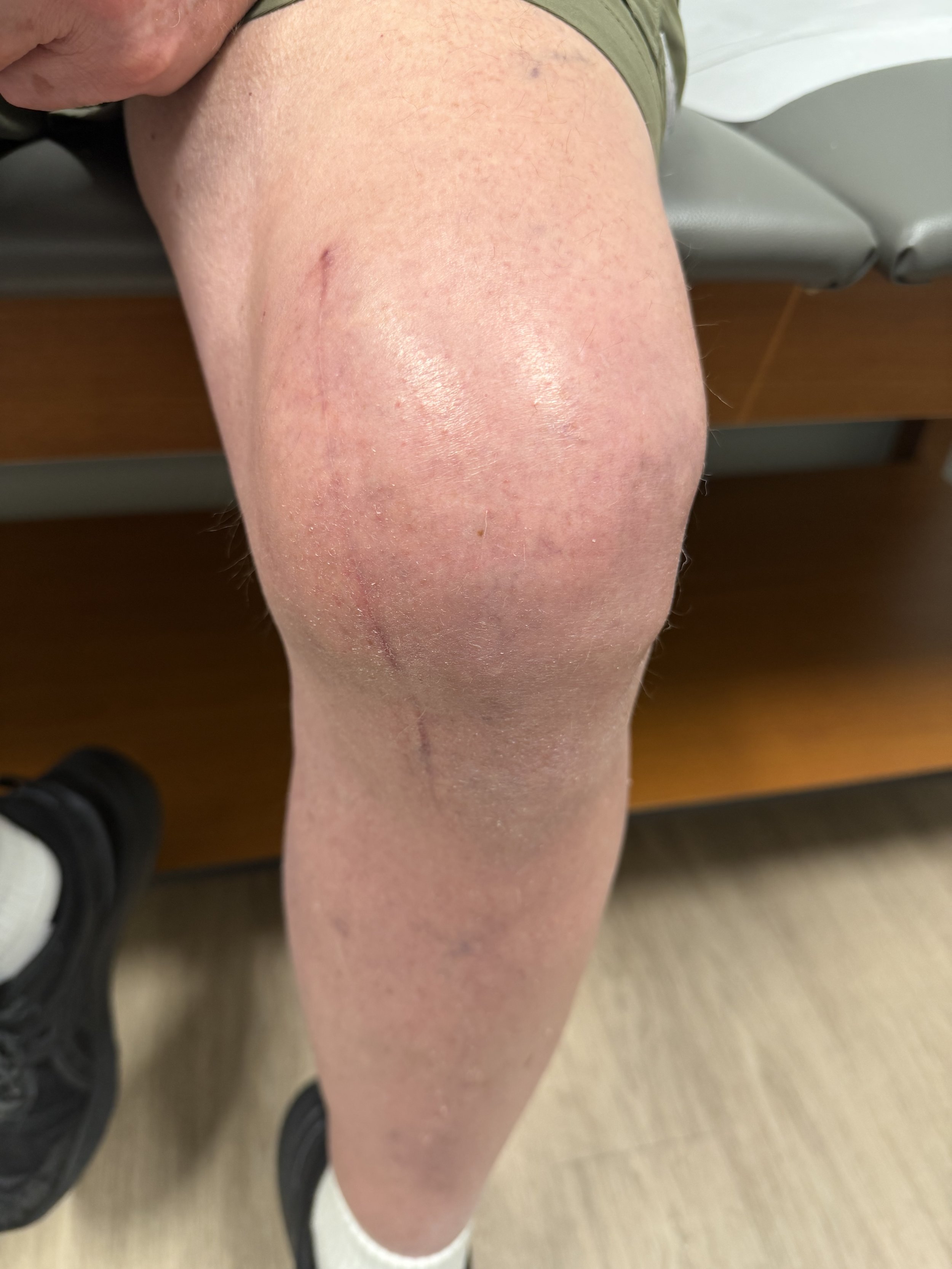

Medial Oblique Incision
2 months post op
Medial Oblique Incision
12 months post op
Key differences in exposure and technique
Tissue plane: The subvastus approach develops a plane beneath (deep to) the vastus medialis muscle rather than incising the quadriceps tendon or splitting the vastus lateralis/medialis fibers. The muscle is gently elevated and retracted medially to expose the joint.
Extensor mechanism integrity: Because the quadriceps tendon and its continuity are maintained, the extensor mechanism is left intact. Traditional medial parapatellar approaches require detachment or incision through the quadriceps tendon or parapatellar retinaculum, and mid-vastus splits muscle fibers.
Patellar handling: The patella is everted much less (often subluxed laterally rather than fully everted) or can be left in place and shifted, reducing traction on the extensor mechanism and patellar blood supply.
Skin and soft-tissue incision: Skin incision is similar in length and location to the medial parapatellar approach, but deeper dissection follows a more medial and submuscular route.
Clinical advantages
Early range of motion (ROM): By sparing the quadriceps tendon and minimizing muscle disruption, patients frequently achieve active knee extension and flexion earlier in the postoperative period.
Less pain and improved function early: Reduced trauma to muscle and tendon correlates with lower early pain and better ability to perform quadriceps activation exercises, transfers, and ambulation.
Faster rehabilitation milestones: Patients often meet early goals (straight-leg raise, independent ambulation with assistive devices) sooner than with approaches that violate the extensor mechanism.
Potentially lower risk of extensor lag: Preserving the quadriceps continuity reduces the chance of postoperative weakness or extensor lag attributable to tendon/muscle injury.
*Individual results may vary
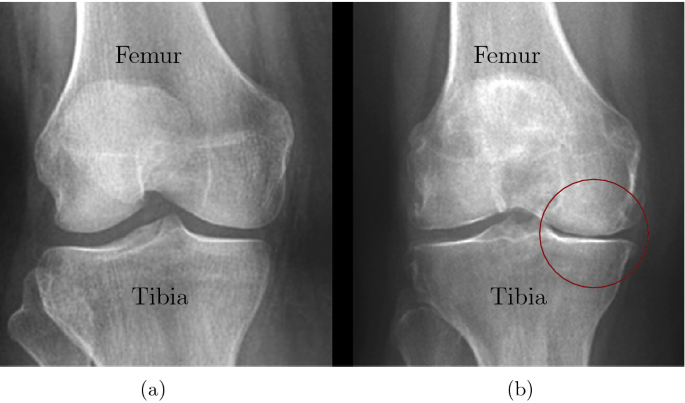
Arthritis is a process that involves the gradual loss of cartilage. To give you a simple analogy, think of it as wearing the tread off the tires on your car. If you put enough miles on your tires, the tires will wear all the tread off. One side of the tire may wear more than the other, just like one side of your knee may wear out before the other side. Patients will often ask “why is my knee hurting so much now if arthritis has been there for a long time?”. I’ll answer this using that same tire analogy. You have been wearing those tires down for a long time. Your mechanic might have even suggested some new tires because some were worn down completely, but you keep driving on them until one day you have a blow out. The process took some time, but eventually things fall apart.
A knee replacement would be better called a knee resurfacing. It is a surgical procedure that changes the surface on the end of the thigh bone (femur) and top of the shin bone (tibia). A few tools are used to remove the worn surface of the bone and then reshape the bone to fit the new metal implants. The implants are typically cemented to the bone and allow you to walk on it the same day. Most of our patients go home the same day as the procedure unless they have significant medical issues.
Phone: 706-839-4096
Anterior Total Hip Replacement
A total hip replacement is a surgical procedure that removes the damaged or worn parts of the hip joint and replaces them with artificial components (a metal or ceramic ball and a plastic or metal socket) to restore smooth, pain-free movement. It is most commonly done for severe arthritis, fractures, or other conditions that cause chronic hip pain and loss of function. The operation is performed under anesthesia, and most patients spend a few days in the hospital followed by a rehabilitation program to regain strength and mobility. Long-term outcomes are generally excellent, with many patients returning to daily activities and reduced pain.

An anterior hip replacement (direct anterior approach, DAA) is a surgical technique for total hip arthroplasty that accesses the hip joint from the front of the leg. Compared with posterior, lateral (anterolateral), or other approaches, the anterior approach offers several potential benefits:
Muscle-sparing technique
The anterior approach uses an intermuscular and internervous plane, typically avoiding detachment of major hip-stabilizing muscles (gluteus medius, piriformis). This preservation can reduce soft-tissue trauma and help maintain hip stability.
Lower early dislocation risk
Because the posterior capsule and external rotators are not routinely cut, anteriorly performed hips often show a lower early postoperative dislocation rate compared with traditional posterior approaches.
Faster early functional recovery
Many patients achieve quicker early milestones—less pain with initial ambulation, earlier independence with gait and transfers, and faster return to basic activities—attributed to less muscle disruption and smaller immediate functional deficits.
Shorter hospital stays and quicker rehabilitation
On average, patients undergoing anterior hip replacement can have shorter inpatient stays and may be more likely to qualify for same-day or next-day discharge, facilitating faster transition to outpatient or home-based recovery.
Smaller early pain and opioid needs
Early postoperative pain scores and short-term opioid consumption may be lower after anterior approaches in some studies, reflecting reduced soft-tissue trauma.
Improved early gait mechanics
Because abductors and external rotators are preserved, patients frequently demonstrate more normal gait patterns earlier in recovery, with less limp or Trendelenburg sign in the short term.
More accurate component positioning (potentially)
The anterior approach, especially when combined with intraoperative fluoroscopy can facilitate visualization and intraoperative imaging for cup orientation and leg-length assessment, improving component positioning and minimizing leg-length discrepancy.
Smaller or cosmetically favorable incision placement
The incision is placed on the front of the hip and can be smaller or more discreet for some patients, which some prefer cosmetically.
Phone: 706-839-4096