Sports Medicine
Expert Care for Sports Injuries & Active Lifestyles
Whether you’re a competitive athlete, weekend warrior, or simply staying active, injuries can disrupt your routine and quality of life. My goal is to provide an accurate diagnosis, personalized treatment, and efficient recovery plans to help you safely return to the activities you enjoy.
I specialize in both non-surgical and surgical treatment of sports-related injures involving the knee, shoulder and other joints

Dr. Wheeler completed an additional year of training in Orthopedic Sports Medicine after his residency to gain specialized expertise in minimally invasive arthroscopic techniques.

Shoulder instability/Dislocations
Frozen Shoulder
Tendon Injuries (Patellar & Quadriceps Tendon)
Phone: 706-839-4096
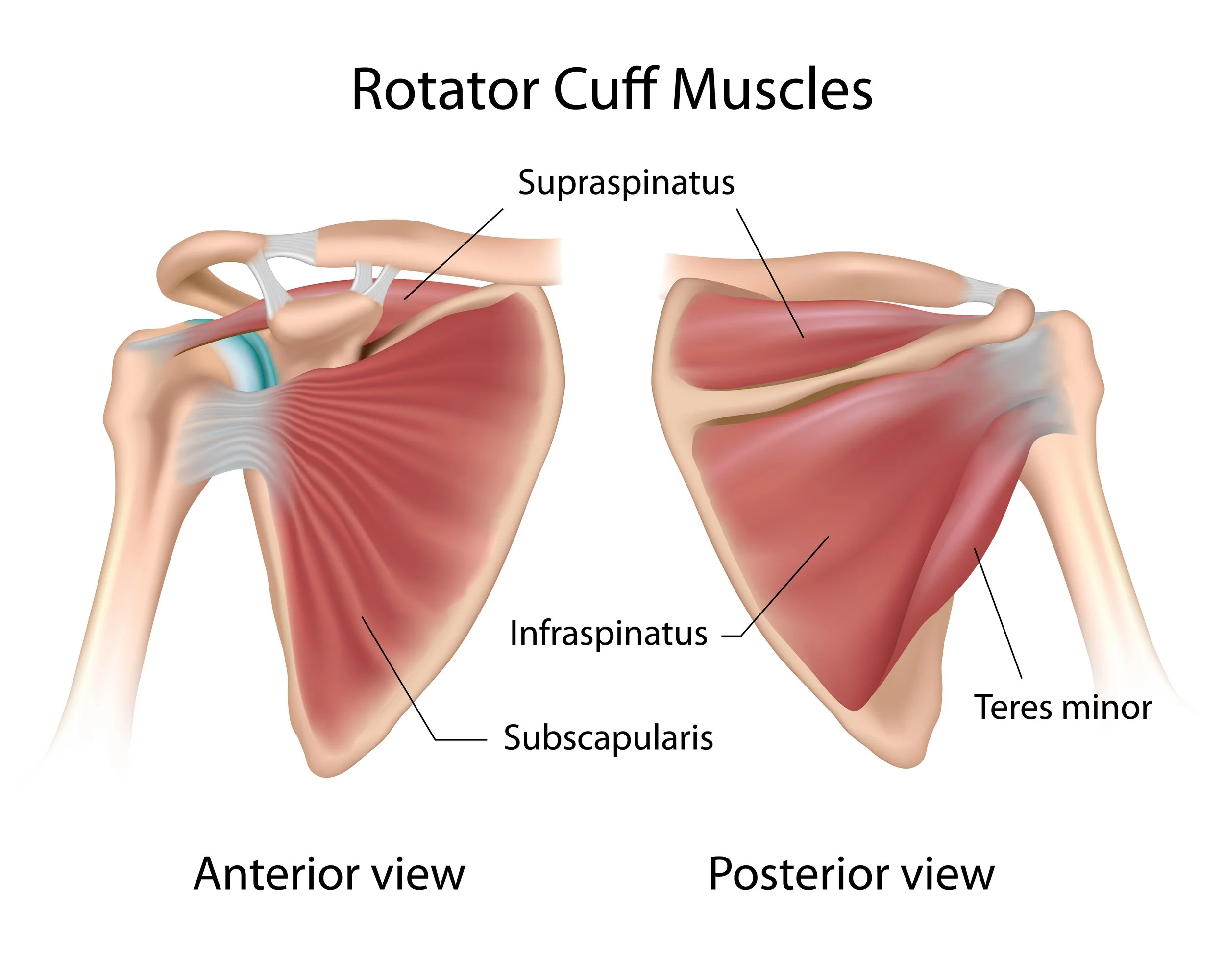
Rotator Cuff Tears
Your rotator cuff is a group of 4 muscles that become tendons that attach to your upper arm to help you move your shoulder
Rotator cuff tears may develop overtime (wear and tear) or because of acute injuries. If these tears are associated with significant pain and loss of function, non-operative treatments are typically initiated. If symptoms do not improve with non-operative care or if an MRI has revealed a tendon tear greater than 50% of the tendon thickness, surgical treatment options will usually be discussed.
Treatment of Full Thickness Rotator Cuff Tears
Non-operative treatments
Activity modifications
Over-the-counter or prescription medications
Subacromial injections
Physical therapy
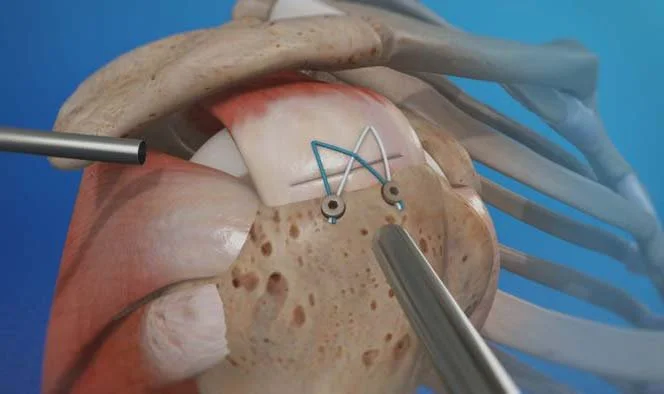
Full thickness tears are treated arthroscopically with a double row repair using small anchors to pull the tendon back to its attachment site
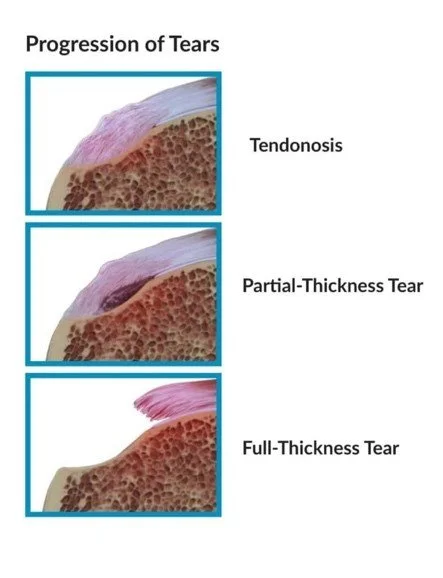
Treatment of Partial Thickness Tears
Partial thickness rotator cuff tears are treated by either:
Conversion to a full thickness tear and then tendon repair utilizing anchors
While this may sound counterintuitive, in some cases this is the best treatment to allow for more predictable tendon repair
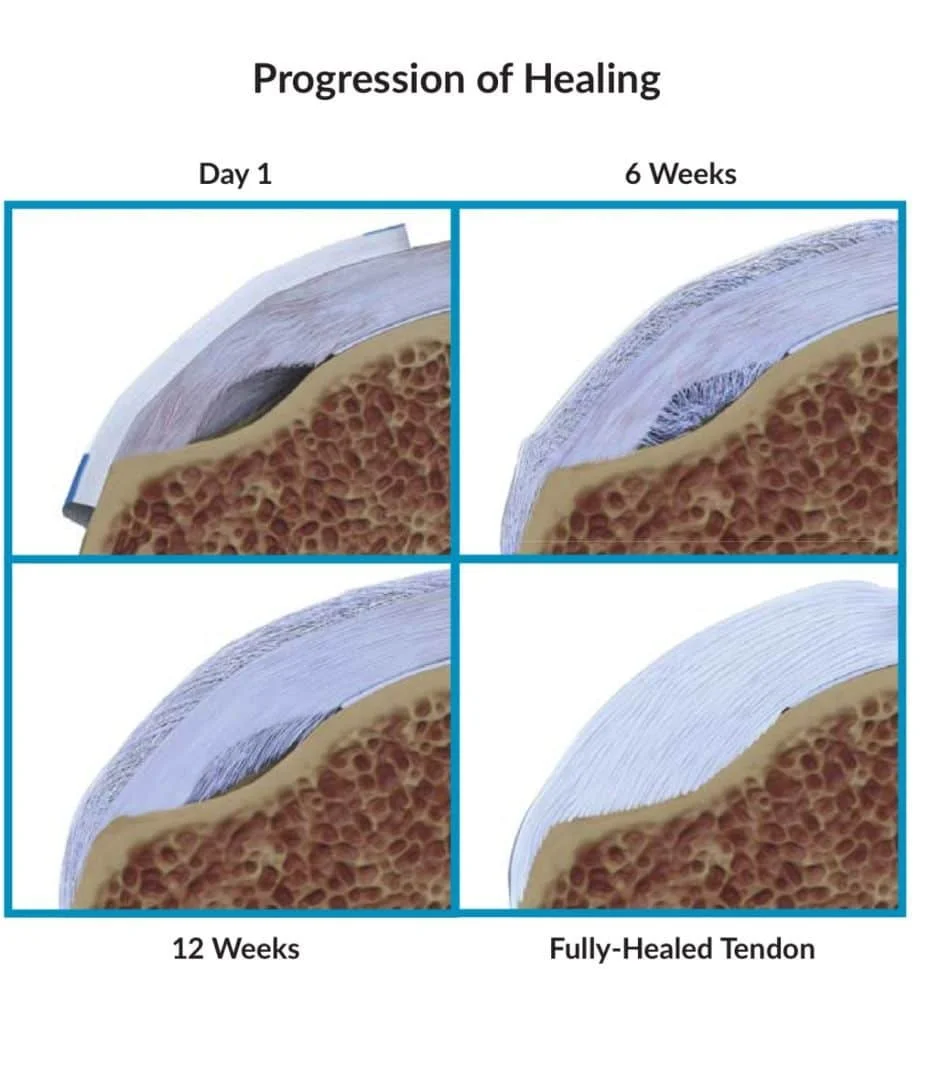
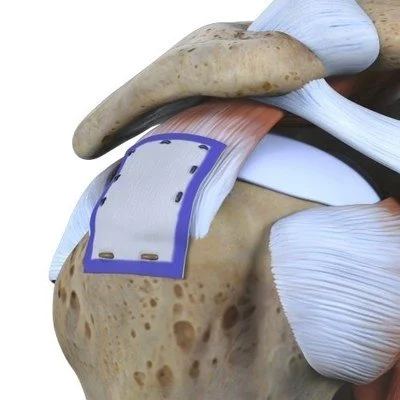
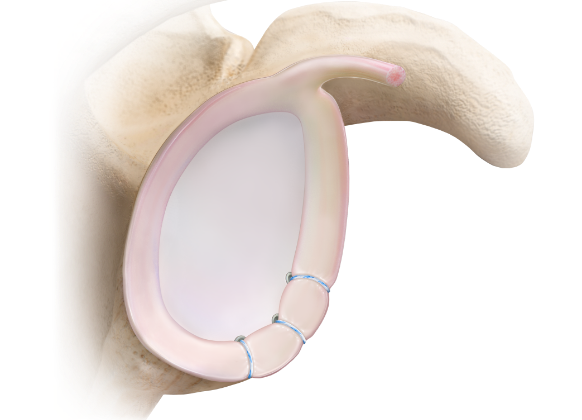
Repair with a Biologic Collagen Patch, such as the Regeneten Bioinductive Implant by Smith and Nephew.
This patch acts as a scaffold to support healing and strengthen the tendon without the need to fully complete the tear.
This technique typically allows for an accelerated recovery
Rotator cuff surgery using minimally invasive arthroscopic techniques
Rotator Cuff Repair with Augmentation
Rotator cuff repair with Augmentation:
During an arthroscopic full thickness rotator cuff repair, a bioinductive collagen implant, such as the Regeneten Bioinductive Implant by Smith & Nephew is placed over the site of the repair. This implant, made from highly purified Bovine tendon, encourages the bodies natural healing response by stimulating new tendon growth. This implant is a scaffolding that your tendon grows into leading to improved tendon thickness and improved function.
Regeneten Bioinductive Implant by Smith & Nephew
Phone: 706-839-4096
Quadriceps Tendon ACL Reconstruction
The anterior cruciate ligament (ACL) is one of the primary stabilizing ligaments of the knee. It is a dense, fibrous band of connective tissue that runs diagonally in the center of the knee, connecting the femur (thigh bone) to the tibia (shin bone).
Primary functions of the ACL:
Resists anterior translation of the tibia relative to the femur (prevents the tibia from sliding forward).
Provides rotational stability, especially limiting internal rotation of the tibia and controlling pivoting or twisting motions.
Clinically, ACL integrity is essential for dynamic activities that involve cutting, pivoting, jumping, and sudden deceleration.
ACL injury commonly results in a sense of instability, swelling, and functional limitation; complete tears often require surgical reconstruction in active patients to restore stability and protect other knee structures (menisci and articular cartilage).
We recommend surgery to reconstruct the ACL if your knee feels unstable or if it is giving way. If you are having episodes of instability, this will place excessive stress on other structures like the articular cartilage and/or meniscus in your knee and will likely lead to earlier degenerative changes than normal.
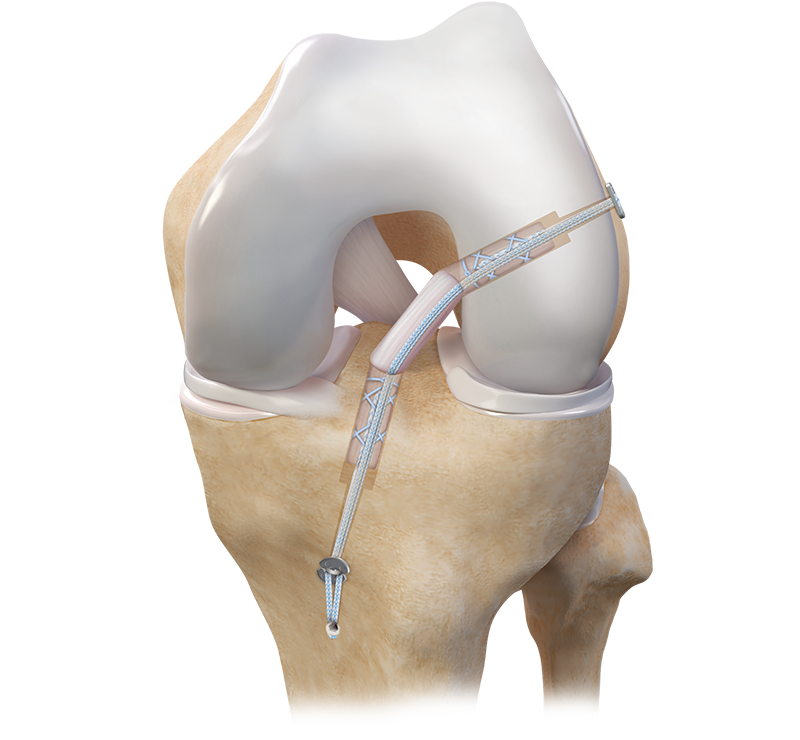
ACL Reconstruction with Arthrex Tightrope and Quadriceps tendon
Autograft (your tendon)
Jogging 4 months
Low-level Agility 5-6 months
Cutting 6-7 Months
Return to Sport 10+ months
Allograft (donor tendon)
Jogging 4 months
Low-level Agility 6-7 months
Cutting 7-8 Months
Return to Sport 12 months
Timelines are estimated based upon current literature studying graft healing and patient progress in formal physical therapy. Concomitant procedures such as a meniscal repair may delay the timeframes listed above.
Phone: 706-839-4096

Shoulder Labral Tears
Overview
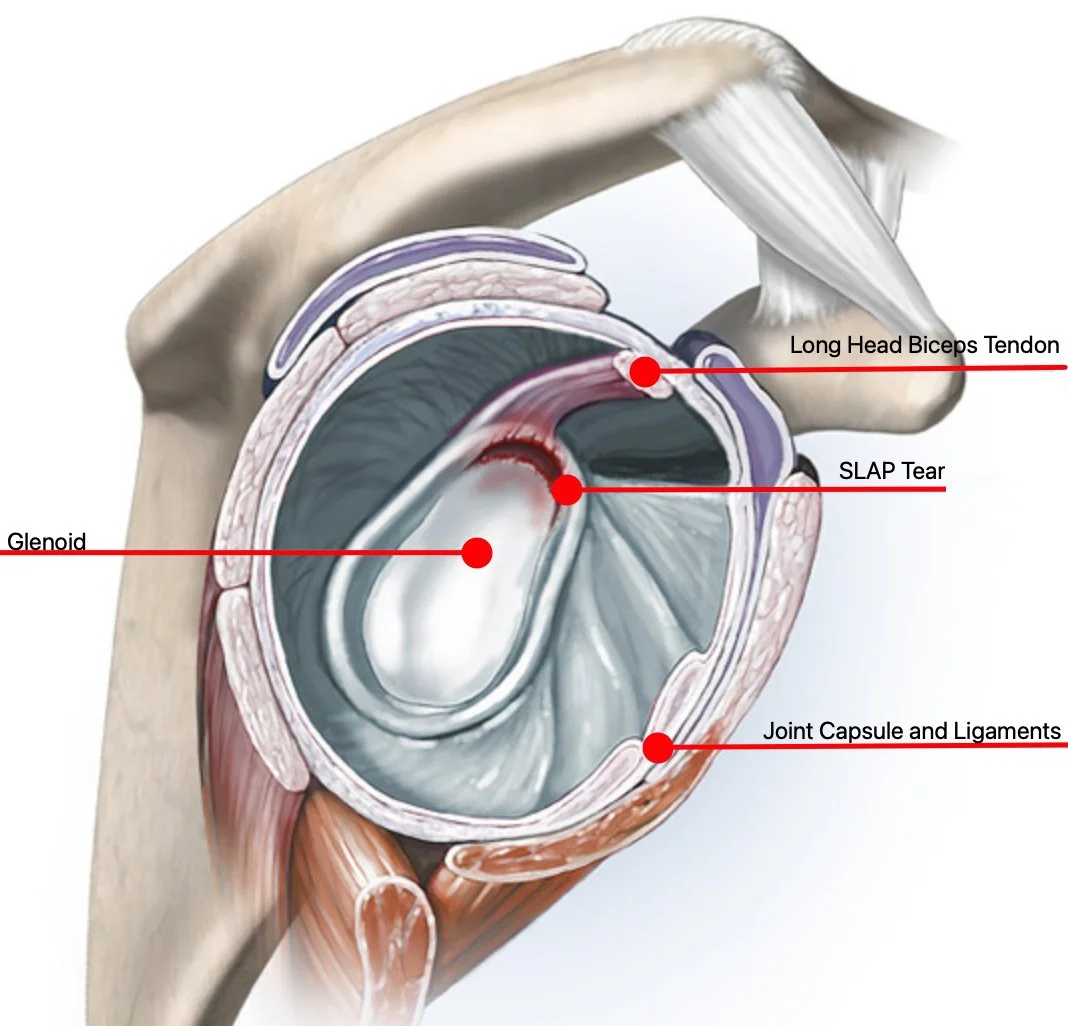
The shoulder is a complicated joint that allows an incredible range of motion. The shoulder joint consists of the humeral head (ball) and the glenoid (socket).
The labrum is a small rim of cartilage that acts to deepen the glenoid and keep the shoulder from dislocating. At the top part of the glenoid, one of the two biceps tendons originates off the labrum and runs along the top of the humeral head and into the arm.
Causes
Injuries to the superior labrum are very common, especially in throwers and active athletes. These injuries are commonly called “SLAP” tears (Superior Labrum Anterior and Posterior). Injuries either occur from repetitive activity such as throwing or serving in tennis, or from a fall onto the shoulder. Labral injuries are commonly seen along with shoulder separations as well.

Diagnosis
Patients with labral tears often complain of pain with overhead activity, pain with lifting heavy objects, and inability to perform well in sports.
The diagnosis of labral tears is made by the patients’ history and physical exam. An MRI is often performed to confirm the diagnosis, and can be very helpful in determining the type of labral injury. The MRI is sometimes performed with a small amount of dye placed into the joint (arthrogram).
Treatment
Treatment for the labral tear usually starts with Physical Therapy and anti-inflammatory medication. However, if this fails, then a surgical option should be discussed. The operation, done arthroscopically, is designed to repair the torn labrum. This is done with small anchors attached to sutures and the labrum is repaired. Initial rehabilitation is about 3 months but most patients will not be allowed to throw until 6-9 months.
Phone: 706-839-4096

Patella Instability
What is Patella Instability?
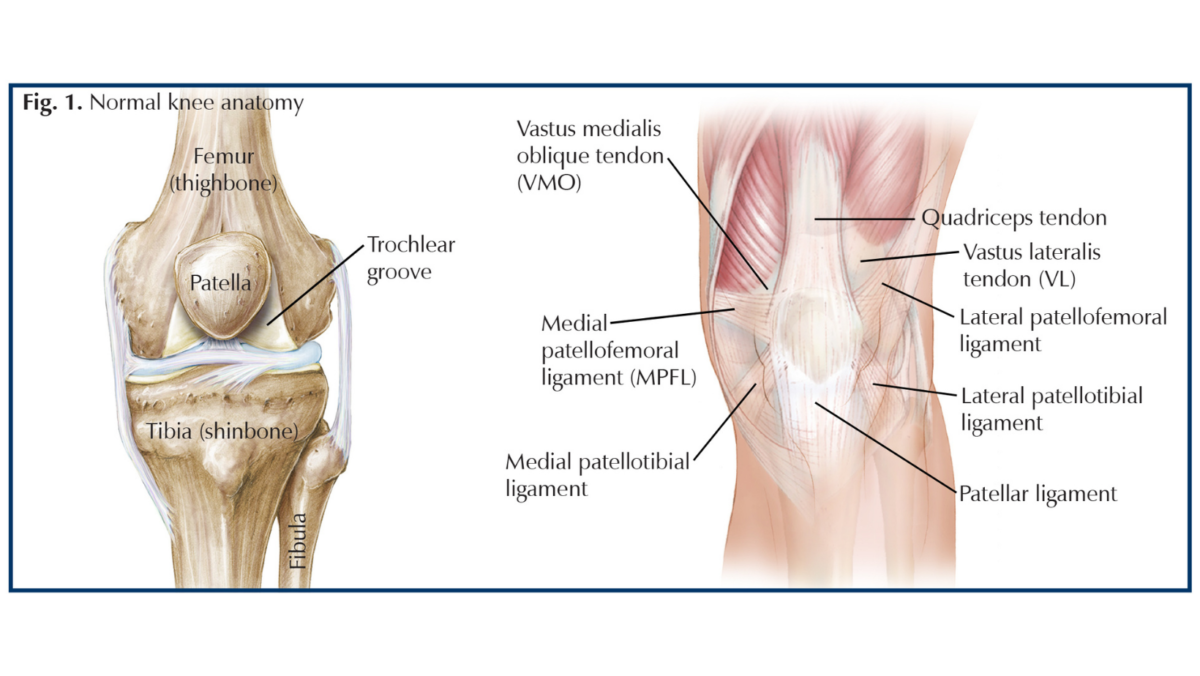
Patellofemoral instability means that the patella (kneecap) moves out of its normal pattern of alignment. This malalignment can damage the underlying soft structures such as muscles and ligaments that hold the knee in place.
Causes of Patellofemoral Instability
Patellofemoral instability can be caused because of variations in the shape of the patella or its trochlear groove as the knee bends and straightens. Normally, the patella moves up and down within the trochlear groove when the knee is bent or straightened. Patellofemoral instability occurs when the patella moves either partially (subluxation) or completely (dislocation) out of the trochlear groove.
A combination of factors can cause this abnormal tracking and include the following:
Anatomical defect: Flat feet or fallen arches and congenital abnormalities in the shape of the patella bone can cause misalignment of the knee joint.
Abnormal Q angle: The high Q angle (angle between the hips and knees) often results in maltracking of the patella such as in knock knees.
Patellofemoral arthritis: Patellofemoral arthritis occurs when there is a loss of the articular cartilage on the back of the kneecap. This can eventually lead to abnormal tracking of the patella.
Improper muscle balance/Quadriceps Malalignment: Weak or externally rotated quadriceps (anterior thigh muscles) can lead to abnormal tracking of the patella, causing it to subluxate or dislocate.
Young, active individuals involved in sports activities are more prone to patellofemoral instability.
Symptoms of Patellofemoral Instability
Patellofemoral instability causes pain when standing up from a sitting position and a feeling that the knee may buckle or give way. When the kneecap slips partially or completely you may have severe pain, swelling, bruising, visible deformity and loss of function of the knee. You may also have changes in sensation such as numbness or even partial paralysis below the dislocation because of pressure on the nerves and blood vessels.
Diagnosis of Patellofemoral Instability
Your doctor evaluates the source of patellofemoral instability based on your medical history and a physical examination. Other diagnostic tests such as X-rays, MRI, and CT scan may be ordered to determine the cause of your knee pain and to rule out other conditions.
Conservative Treatments for Patella Instability
If your kneecap only partially dislocates (subluxation), conservative treatments with Physical therapy and braces may help your symptoms. If you have complete instability with dislocations of the patella, surgical treatment is indicated.
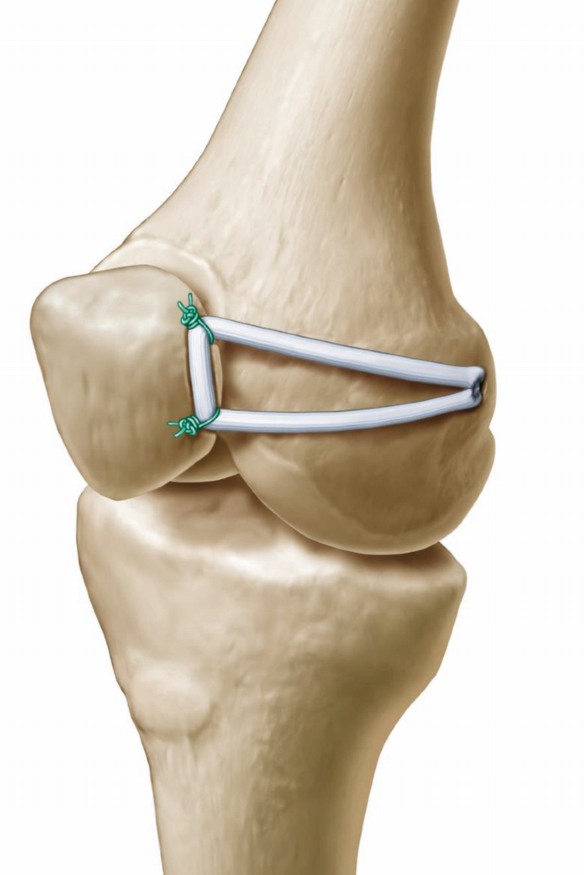
Surgical Treatments for Patellofemoral Instability
The type of surgery depends on your exact circumstances. In situations where the bony anatomy is normal, but a severe injury has resulted in a tear of ligaments that provide stability to your kneecap, those ligaments will be reconstructed with donor tendons. The medial patella femoral ligament (MPFL) is a ligament on the inside (medial) side of your knee that acts to prevent the patella from moving too far lateral (to the outside) and is typically torn if your kneecap has dislocated. A MPFL reconstruction is a surgical procedure that involves rebuilding that ligament with a donor tendon.
In some cases, the underlying bony anatomy may a contributing factor to the patella dislocating and therefore should be addressed during the surgical procedure. The most common bony abnormalities are an underdeveloped groove for the patella to sit in or an abnormal Q angle (knock knees). These issues will be assessed with an MRI during the workup.
In cases where the malalignment is severe, a procedure called a tibial tubercle osteotomy (TTO) will be performed. In this procedure, a section of bone where the patellar tendon attaches to the tibia is removed. This bony section is then shifted and properly realigned with the patella and reattached to the tibia using screws. Once the malalignment is repaired and confirmed with arthroscopic evaluation, the incisions are closed with sutures.
Postoperative Care Following Treatment of Patellofemoral Instability
The postoperative instructions will depend on the exact surgical procedure performed, but typically requires crutches for 1-2 weeks and a postoperative knee brace that allows us to control how much range of motion your knee is able to perform. As you get further from your surgery, the brace is adjusted to allow your knee to bend more. The brace is typically discontinued around 2 months postop.

Phone: 706-839-4096

Meniscus Injuries
Knee pain can make everyday activities—walking, climbing stairs, exercising, or even standing—difficult and limit your independence and quality of life. A common cause of knee pain is a meniscus tear, a cartilage injury that can cause pain, swelling, catching, and reduced range of motion. Prompt evaluation and appropriate treatment can relieve symptoms, restore function, and help you return to the activities you enjoy.
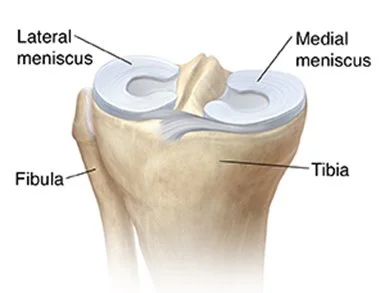
What is a Meniscus?
The meniscus is a shock absorbing cartilage disc on both sides of the knee.
What are the symptoms of a meniscus tear?
Symptoms of a meniscus tear that may include the following:
Pain in the side or center of the knee
Recurring knee pain/pain that comes and goes
Clicking feeling or sound in the knee
Knee stiffness
Immobility/inability to walk
Inability to straighten the knee
Knee instability or “knee giving out”
How does a meniscus tear occur?
A meniscus tear may occur with an injury or sometimes degenerative tears occur with normal everyday activities.
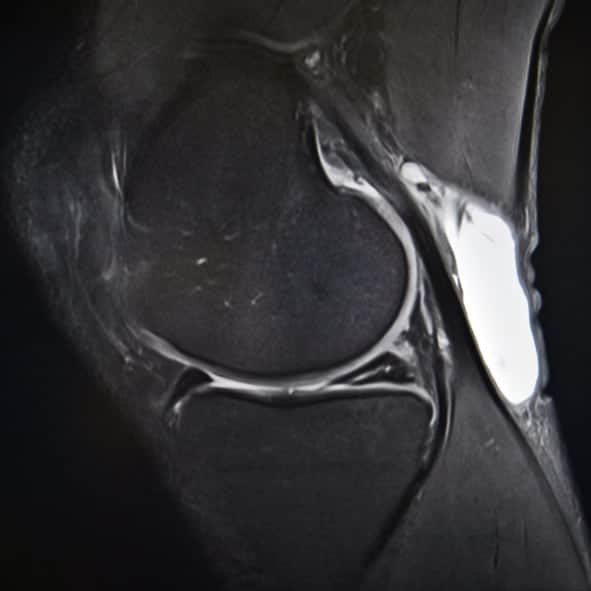
Sagittal view of knee demonstrating tear of the posterior meniscus (tan arrow) with a bakers cyst present
Do meniscus tears require surgery?
Not all meniscus tears require surgery. Some tears heal on their own, and others may stop causing symptoms even without full healing. When tears improve, patients typically notice reduced pain and better function within 4–6 weeks. Treatment during this period often focuses on symptom management by activity modification and anti-inflammatory measures. If pain, swelling, or mechanical problems persist beyond this timeframe, further evaluation and discussion of surgical options may be warranted.
How are meniscus tears diagnosed?
Meniscus tears are typically diagnosed by a combination of physical exam findings and an MRI.
Surgical treatments for meniscus tears include minimally invasive knee arthroscopic techniques
If conservative RICE practices and subsequent physical therapy to strengthen the surrounding muscles that support your knee have not alleviated your knee pain, or if your knee locks, it is likely time to pursue arthroscopic knee surgery.
If the tear can’t be repaired, the torn area can be trimmed away so that it no longer catches on surrounding bone and tissue when you move your knee.
These are minimally invasive procedures that take on average about 15 minutes to perform, and they can dramatically improve your knee function and reduce pain.
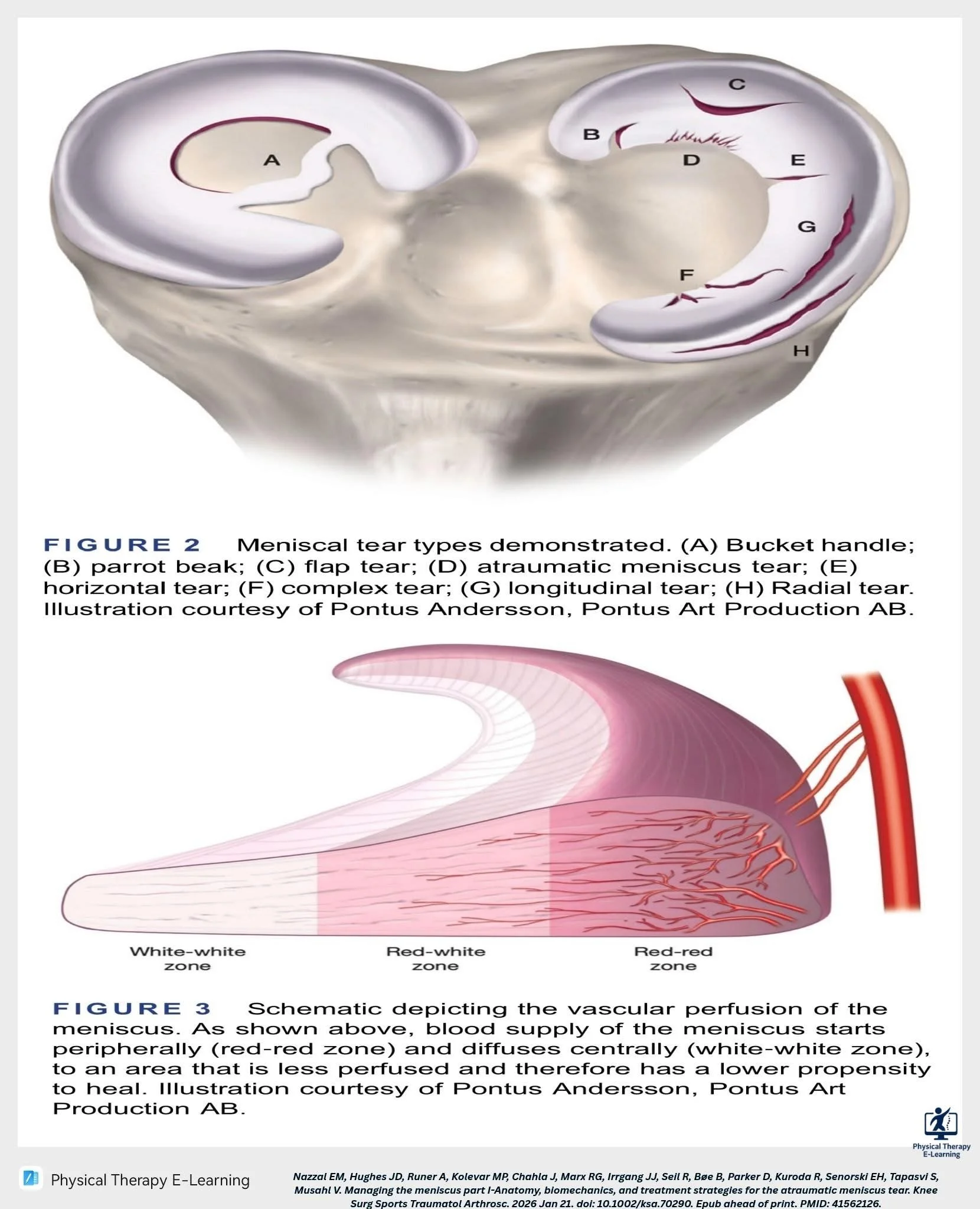
Figure 2: Meniscus tear types
Figure 3: Blood supply to the meniscus
How long is the recovery after a meniscus surgery?
The recovery depends on whether the tear was repaired (sutured) or if the torn parts were trimmed (meniscectomy). With a repair a brace and crutches will be necessary to protect the repair for 4 to 6 weeks. If the meniscus tear was trimmed, you will typically use crutches for 2 days and can weight bear immediately as tolerated.
The decision to repair versus trim is based on several factors including age of the patient, tear configuration, and tear location (zone with good or limited blood supply)
Phone: 706-839-4096
Cartilage Reconstruction

Matrix-induced autologous chondrocyte implantation (MACI) is a surgical treatment designed to repair focal cartilage defects in joints, most commonly the knee. MACI uses a patient’s own cartilage cells (chondrocytes) grown on a biodegradable scaffold that is implanted into the damaged area to restore hyaline-like cartilage, reduce pain, and improve joint function.
How MACI works
Cartilage biopsy: A small sample of healthy cartilage is arthroscopically harvested from a non-weightbearing area of the joint.
Cell expansion: Chondrocytes are isolated from the biopsy and cultured in a laboratory for several weeks to increase cell number.
Scaffold seeding: Expanded chondrocytes are seeded onto a porous, bioabsorbable matrix (scaffold) that supports cell distribution and new tissue formation.
Implantation: The scaffold with the patient’s chondrocytes is implanted into the defect and secured. Over time the scaffold degrades while the cells produce new cartilage-like tissue.
How the diagnosis is made
Clinical history and exam: Diagnosis begins with a focused history of joint pain, swelling, mechanical symptoms (catching, locking), a history of trauma, prior cartilage injury, or persistent pain after conservative care. Physical examination assesses joint line tenderness, range of motion, alignment, ligament stability, and signs of meniscal or other intra-articular pathology.
Imaging:
Plain radiographs: Weight-bearing X-rays assess joint alignment, osteoarthritis, and bone changes. Radiographs help exclude advanced degenerative disease.
MRI: Magnetic resonance imaging is the primary modality to confirm a focal chondral defect, define size, depth, location, and evaluate surrounding cartilage, bone marrow, menisci, and ligaments. MRI also helps rule out diffuse arthritic change.
Occasionally CT or CT arthrography: Used when detailed bone morphology or subchondral bone assessment is needed.
Diagnostic arthroscopy: Arthroscopy provides direct visualization and accurate measurement of the defect and can be used to confirm that the lesion is suitable for MACI when noninvasive imaging is inconclusive.
Patient selection considerations: Assessment includes age, body mass index, activity level, alignment, ligamentous stability, meniscal status, and presence of diffuse osteoarthritis. Careful selection improves the likelihood of success.
When MACI is indicated
Suitable lesions: MACI is intended for symptomatic, focal, full-thickness cartilage defects of the joint surface, typically 2 to 10 cm² in size, depending on patient factors and surgeon preference.
Failed conservative care: Indicated when nonoperative management (activity modification, physical therapy, anti-inflammatory medications, injections) has not relieved symptoms.
Failed prior cartilage repair: MACI can be considered after unsuccessful microfracture or other cartilage procedures in selected patients.
Favorable joint environment:
Minimal or no diffuse osteoarthritis. MACI is not appropriate for end-stage degenerative joint disease.
Correctable malalignment: Varus or valgus malalignment should be addressed (for example, with osteotomy) to protect the repair.
Stable ligaments: Instability should be corrected prior to or concurrent with cartilage restoration.
Intact or repairable meniscus: Adequate meniscal function is important to offload the cartilage repair.
Patient factors: Younger, active patients with focal defects and reasonable expectations are the best candidates. Advanced age, high body mass index, or generalized arthritis may reduce the likelihood of good outcomes.
Expected outcomes and recovery
Goals: Reduce pain, improve function, and delay or prevent progression to joint replacement by restoring durable cartilage-like tissue.
Rehabilitation: Postoperative rehab typically includes a period of protected weight-bearing, range-of-motion exercises, progressive strengthening, and a gradual return to sport over 6–12 months depending on the lesion and joint.
Success rates: Many patients experience significant pain relief and functional improvement. Long-term outcomes correlate with lesion size, location, patient selection, and adherence to rehabilitation
Summary: MACI is a biologic cartilage restoration option for properly selected patients with symptomatic focal full‑thickness cartilage defects and a favorable joint environment. Diagnosis involves clinical evaluation, MRI (and sometimes arthroscopy), and assessment of alignment, stability, and meniscal status. MACI is indicated when conservative treatment has failed and when underlying joint factors can be optimized to support a durable repair. Schedule an appointment to determine whether MACI is appropriate for your specific condition and goals.
Osteochondral Autologous Transplantation Surgery (OATS)
Osteochondral autologous transplant (OAT) surgery — also called mosaicplasty — is a procedure that treats focal cartilage defects in a joint by moving small plugs of healthy cartilage and underlying bone (osteochondral grafts) from a non-weight-bearing area of the patient’s joint to the damaged area. Because the grafts come from the same person (autologous), there is no risk of disease transmission or rejection.
When it is indicated
Symptomatic, focal cartilage defects (often in the knee) that have failed conservative care (physical therapy, activity modification, medications, injections).
Typical candidates are younger, active patients with relatively small-to-moderate full-thickness cartilage lesions (commonly 1–4 cm²).
Used when the surrounding joint alignment and stability are adequate; not ideal for widespread arthritis or very large defects.
Goals of the procedure
Restore a durable, hyaline-like cartilage surface at the defect site to reduce pain.
Reestablish joint congruity and load distribution to protect surrounding cartilage.
Improve joint function and return to activity or sport.
Delay or prevent progression to larger cartilage loss and degenerative arthritis.
What to expect in surgery
Performed arthroscopically or with a small open approach.
Small cylindrical plugs (typically 2–10 mm diameter) are harvested from low-load areas and transplanted into prepared sockets at the defect to create a contiguous cartilage surface.
Procedure time and number of plugs depend on defect size.
Recovery timeline (general guide; individual recovery varies)
Immediately after surgery: Crutches and limited weight-bearing on the operative limb as directed (often 4–8 weeks) to protect grafts. Pain managed with medications and ice; wound care instructions provided.
First 2 weeks: Focus on pain control, wound healing, and beginning controlled range-of-motion exercises to prevent stiffness. Emphasis on protecting the graft from load.
2–6 weeks: Gradual increase in passive and active range-of-motion exercises and controlled strengthening. Continue partial weight-bearing per surgeon protocol.
6–12 weeks: Progression of strengthening, balance, and low-impact activities; transition toward full weight-bearing as tolerated and as allowed by imaging/clinical assessment.
3–6 months: Continued strengthening, endurance work, and sport-specific drills begin for many patients; low-impact sports may be possible.
6–12 months: Many patients achieve substantial improvement in pain and function; higher-impact sports return is considered case-by-case, often earliest around 6–12 months depending on defect size, location, and healing.
12 months and beyond: Full activity clearance when graft integration, strength, range of motion, and clinical symptoms are satisfactory.
Discuss specifics with your orthopedic surgeon—indication, expected outcomes, and a personalized rehabilitation plan depend on your lesion size, location, overall joint health, and activity goals.
